For Big Tobacco and Brewers, Grass is Greener
Big Tobacco and Big Alcohol are investing in pot to make Big Marijuana, the New York Times reports this morning.
- Altria, the tobacco company that makes Marlboro and other cigarettes, paid $1.8 billion last week to buy nearly half of Cronos Group, a Canadian marijuana company.
- Constellation Brands, the company that makes Corona and other beers, paid $4 billion last August for a major stake in another Canadian pot company called Canopy Growth.
- And Molson Coors Canada, the Canadian branch of Molson Coors, bought a controlling interest in a joint venture with The Hydropothecary Corporation, a third Canadian pot company.
All three Canadian marijuana companies got their start producing the drug for medical use and are licensed by Health Canada. Canada’s full legalization of marijuana in October opened the door to the recreational market. US companies want an early entry into a market they believe will open soon in the US.
This morning’s print edition of today’s Times has a different title for this story: “This is the Dawning of the Age of Pot, Inc” the headline claims. Apparently, the Age of Aquarius (“Let the Sun Shine In”) has suffered a premature death. Big Tobacco lied to Americans for nearly a century, claiming nicotine is not addictive and smoking is harmless. Even before it became Big, the marijuana industry began following Big Tobacco’s playbook with the same mantra: Is pot addictive? “No.” “Harmless? Yes. It’s even a medicine.”
Sound familiar?
“The arrival of large multinational corporations portends sweeping changes for an industry that until recently operated in the shadows. As billions of dollars pour into product development, marketing and manufacturing, these companies will be looking to create big brands with the market share to match,” notes the Times.
Earlier this year, Coca-Cola representatives acknowledged their company was looking closely at the CBD industry. For a few days, Target sold CBD products online but abruptly ended the practice. Diageo, a spirits company, was rumored to be close to joining forces with an unnamed Canadian pot company last summer, but no announcement has been made yet. And Walmart Canada is looking into the industry but currently has no plans to start selling products containing CBD or THC.
Some CEOs like Coca-Cola’s James Quincey are holding back. “It needs to be legal, it needs to be safe, and it needs to be consumable,” he said on CNBC this week. “It’s not there yet.”
Nonetheless, industry spokesmen say as more big companies get involved with marijuana, they’ll likely pressure Congress to legalize the drug in the U.S. nationwide, like Canada.
So, watch out. Those Green Marlboro packs containing pre-rolled joints seen in counterculture publications may not be hippie hallucinations after all.
Read the New York Times article here.

Here’s what happens when marijuana is commercialized
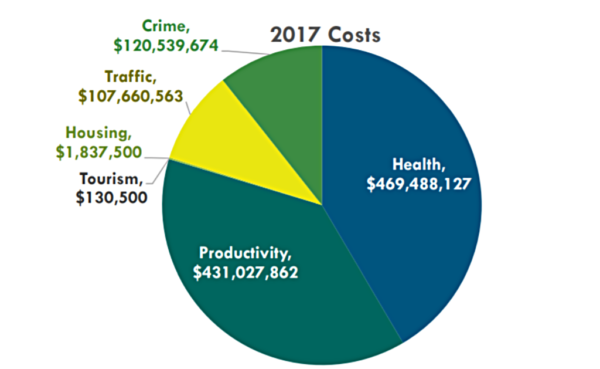
This graph, from a 2018 report by the Colorado Department of Public Safety (state law mandates a comprehensive report every two years), presents the clearest picture yet of what happens when a state commercializes marijuana.
Colorado legalized the drug for medical use in 2000. Patients who obtained a medical marijuana card from the state could access the drug by selecting a caregiver to grow it for them, and caregivers could grow enough marijuana for six patients. The number of patients who obtained cards grew from 94 in 2001 to 4,819 in 2008.
Effective 2009, the Colorado legislature established a system to license people to grow, manufacture, and sell marijuana for medical use. A license meant the holder could start investing in and making profits on these activities. In other words, Colorado created one of the first commercial marijuana businesses in the nation.
In 2008, there were no licensed medical marijuana growers, product manufacturers, or dispensaries in Colorado. By the end of 2012,* there were approximately 1,150 licensed facilities, and the number of patients who obtained medical marijuana cards jumped from 4,819 to 108,526 in four years.
Read more about this on page 157 here.
*Colorado archives licensee data, but they only go back to 2013. These data are taken from January 2013, one month after 2012 ended.

Farm Bill agreement allows nationwide hemp cultivation for any use – including CBD
If the US House passes the Farm Bill this week, hemp will be legal throughout the US. Hemp is defined as containing less that three-tenths of one percent of THC, the cannabinoid in marijuana that makes users high. The Senate passed the bill this week.
CBD products can be made from hemp although, because some patients insist they need THC as well, CBD must be extracted from marijuana to obtain THC.
According to Marijuana Business Daily, the measure would lift restrictions on advertising, marketing, banking, and other financial services on hemp growers and manufacturers. It also would:
- Allow hemp production in all 50 states, including the production of CBD
- Producers who raise hemp with a higher THC level than 0.3 percent would not be guilty of a drug crime but would have to submit a plan to correct the problem
- Allow the sale of hemp and CBD across state lines
- Make the US Department of Agriculture administrator of the program
- Legalize production in US territories and on Indian tribal lands
- Require taxpayers to subsidize the hemp industry by providing access to federal farm support, including crop insurance, federal water access, and low-interest loans to new farmers
- Allow hemp producers to bring “foreign nationals” to the US to fill “temporary agricultural” jobs
- Remove barriers to obtaining patents and trademarks
- Ban state or federal drug felons from participating in the program for 10 years, and
- Require the agriculture department to work with the Attorney General on hemp rules.
Read Marijuana Business Daily article here.

Maryland marijuana panel approves ban on cannabis advertising on billboards, radio, TV, and other media
The Maryland Medical Cannabis Commission voted unanimously to ban nearly all advertising of marijuana for medical use. The industry says it will fight the ban when the General Assembly convenes in January 2019. The rules prohibit advertising on or in:
- Billboards
- Radio
- Television
- Most online outlets
- Newspapers and magazines that cannot prove 85 percent of their audience is over age 18
- Leaflets or flyers in most public and private places
- Internet ads must include an age verification page.
An industry spokesman claimed the ban came about after a billboard showing Adam and Eve smoking a joint upset two legislators. However, a spokeswoman for the commission said the effort was to mirror bans on tobacco advertising.
A deputy attorney general asked the commission to also add specific language prohibiting manufacturers from making any medical claims without scientific evidence.
The new rules state that marijuana companies may not make any claim that is “false or misleading in any material way or is otherwise a violation” of state laws.
Read The Baltimore Sun story here.
EDITORS NOTE: This column with images is republished with permission.