Immigration reform “starts” with securing the wide open southern border and while at the same time to finally enforcing Federal Immigration Laws. The 9/11 Commission recommended, in order to prevent terrorists from viciously attacking the Republic in the future, as the illegal aliens who were terrorist hiding in plain sight throughout America did on September 11, 2001, that the United States Citizenship and Immigration Service, Ice, and the Border Patrol should enforce Federal Immigration Laws and control the borders of the United States like every other nation in the world does. Fifteen years after 9/11 Congress and Obama have refused to secure the borders. Obama has issued orders to the U.S. Border Patrol and ICE Agents to cease apprehending and deporting Illegal Aliens and has cancelled the Secure Communities Program that automatically checked state and local incarcerated inmates against the list of Illegal Aliens listed in the Federal Databases to see .if certain inmates should be picked up by ICE for deportation.
Because of the wide open southern border, the current outbreak of measles is the worst measles epidemic in 60 years and is spreading throughout the US. WND reviewed the history of measles outbreaks in the US since 1980, and after careful evaluation, determined that almost all of the outbreaks came from overseas, and that California had some of the largest concentrations of measles, as well as the largest influx of Illegal Aliens from across the wide open southern border. For 6 years the Obama administration has refused to follow the required medical testing and examining procedures required to determine if any Illegal Alien crossing the wide open border had infectious diseases.
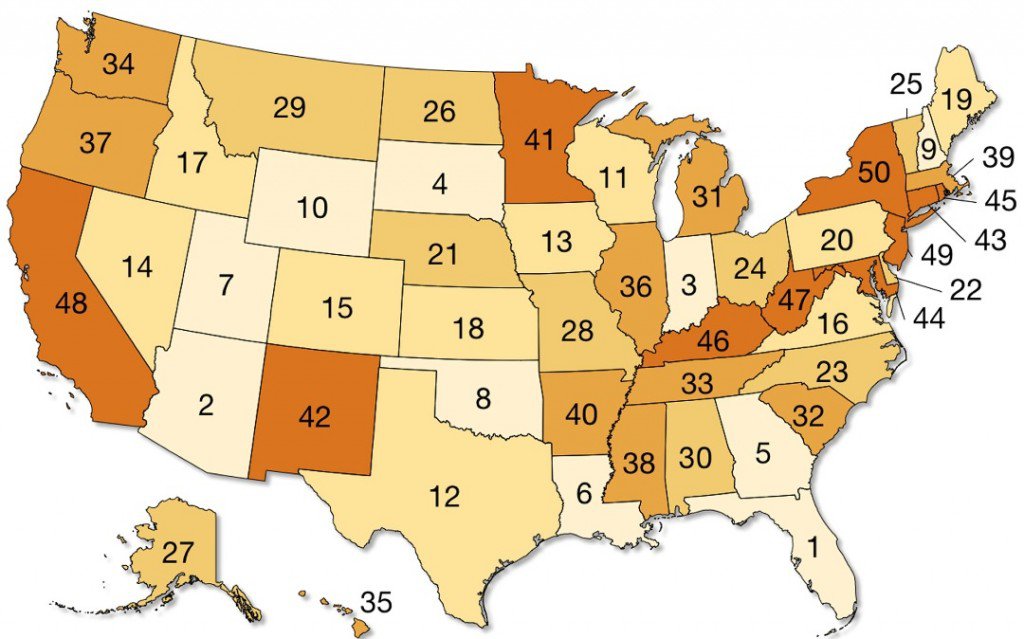
The Obama administration blamed the current worst measles epidemic in 60 years on Disneyland, instead of on its flagrant violation of Federal Immigration Quarantine Laws. Measles did not spread to 27 states from Disneyland, it is another of the many lies promulgated by the Obama administration that is being reported by the left of center liberal media establishment (illegal alien children from Central American may have been taken to Disneyland for recreation, and may have infected some Americans children visiting there), Most of the Illegal Alien children from Central America who flooded across the wide open southern border were released by Border Patrol Agents “unscreened” to travel to over 27 states within 72 hours of their apprehension at the southern border. Some of those infected Illegal Alien children even passed infectious diseases on to Border Patrol Agents.
The Center for Disease Control and Prevention (CDC) has reported that they have seen an alarming spike in measles since 2014, with a record of 644+ cases in 27 states (that is a very old number, but the updated numbers of cases are being covered up by CDC). Dr. Anne Schuchat of the CDC told reporters, “We don’t know exactly how this measles outbreak started, but we think it was likely people infected with measles overseas.” Obama appointees at CDC have refused to pinpoint the origin of the reported uptick of 644+ cases of measles in 27 states. Hundreds of thousands of Illegal Alien children from Central America walked across the wide open southern border and are still doing so. Those Illegal Alien were never processed thru an Immigration Detention Center, as required by Federal Immigration Laws, so they could be tested and examined by Medical Professionals to determine if they were carrying infectious diseases. If that were done and they tested positive, they should have been quarantined as required by Federal Immigration Laws instead of being released to the general public. Even US Astronauts are quarantined when they return from outer space.
Popular radio talk show host Michael Savage who holds a Ph.D. degree in nutritional ethnomedicine said:
The Socialist Government, media, academia, medical apparatchiks have looked the other way or changed the origin of numerous illnesses which were once eradicated in our once-first world nation.” Since the massive influx of Illegal Alien children from Central America, who were not being medically screened, the United States has had outbreaks of numerous illnesses that were once eradicated such as dangerous strains of Flu, Scalia, TB, Measles, Mumps, Rubella, Smallpox, Leprosy, and even Malaria—their outbreaks have been covered up by the Obama appointees at CDC. Every day, the Obama administration continues to violate Federal Immigration Quarantine Laws, infectious diseases will continue to infect the general population and children who are required to go to grammar schools along with Illegal Alien children from Central America.
Numerous epidemics sweep Central America, and an aggressive mosquito transmits the deadly enterovirus (EV-D68) and yellow fever, and some infectious diseases are transmitted by insects, including the spread dengue fever. EV-D68 has been responsible for at least 14 deaths in the US over the last 12 months. Please read the below listed article about Illegal Aliens bringing many infectious diseases into the U.S. like measles, enterovirus (EV-D68), dengue fever, dangerous strains of Flu, Scalia, TB, Mumps, Rubella, Smallpox, Leprosy, and even Malaria. Some Illegal Alien children transport mosquitos that are carrying very dangerous infectious diseases, in their clothing. The Obama administration’s continues to violate Quarantine Laws, in order to facilitate the massive illegal entry of Illegal Aliens, thru the southern border of the United States. That practice has created a public health hazard for children enrolled in grammar schools and for the general public in communities throughout the United States.
Any member of Congress or any candidate for President in 2016, who doesn’t support closure of the Southern Border, doesn’t support enforcement all Federal Immigration Laws & Regulations, and those who support Obama’s Executive Orders to issue Work Permits and Social Security Numbers for 5 million Illegal Aliens and for 1.5 million Dreamers, should be defeated at the polls in November 2016.
For 6 years, Obama has proclaimed how much he cares about American union workers, low income Americans, and middle income taxpayers, yet he is doing all he can to issue 6.5 million Work Permits and Social Security Numbers for Illegal Aliens and Dreamers, despite the fact that Obama has been restricted by U.S. Federal Court from issuing Work Permits and Social Security Numbers. If that occurs those 6.5 million Illegal Aliens will take jobs away from the 100 million unemployed low income Americans, union workers, and middle income taxpayers. Those 6.5 million Illegal Aliens will seek to obtain drivers licenses, in violation of Federal Laws, so they can illegally register to vote in 2016.
EXCLUSIVE
‘So these problems are going to be coming to your town’
AARON KLEIN
Is there more to the measles outbreak than the Centers for Disease Control and Prevention have acknowledged?
A close look at the history of measles outbreaks in the U.S. over the last 15 years evidences two significant themes – the vast majority of all cases were imported from outside the country, and many of the disease clusters were located in California, a state known for its large concentration of illegal aliens.
Still, while diseases such as enterovirus are rampant in the countries where most illegal aliens originate, there does not appear to be strong evidence that current or past measles outbreak originated with illegal aliens.
The medical debate has entered the political arena. Rep. Mo Brooks, R-Ala., and radio host Rush Limbaugh have suggested a connection between illegals and the spread of disease, including measles.
Brooks stated last week: “I don’t think there is any health-care professional who has examined the facts who could honestly say that Americans have not died because the diseases brought into America by illegal aliens who are not properly health care screened, as lawful immigrants are.”
Brooks said it “might be the enterovirus that has a heavy presence in Central and South America that has caused deaths of American children over the past six to nine months, it might be this measles outbreak – there are any number of things.”
That same day, Limbaugh told his audience: “We have a vaccination problem for one reason: Barack Hussein Obama and his open-borders immigration policy, which opened the southern borders to children sick, healthy, you name it, poor, ill-educated, just tens of thousands of kids flooded the southern border all of last year.
“They were never examined before they got here,” Limbaugh said. “They were never examined after they got here and quarantined if they had a disease. They were just sent out across the country. Many of them had measles.”
In a conversation on CNN that focused on measles and other diseases, presidential hopeful Dr. Ben Carson spoke generally about illegal aliens bringing in illnesses while not directly attributing the measles current outbreak specifically to them.
Illegals ‘slipping through cracks’ with diseases
PolitiFact points out the Office of Refugee Resettlement’s protocol calls for it to provide “vaccinations to all children who do not have documentation of previous valid doses of vaccine.”
However, PolitiFact misses the fact that the Refugee Resettlement, a program of the Department of Health and Human Services, mostly deals with legal immigrants who obtain the status of refugee and who are seeking safe haven within the U.S.
The HHS’s Administration for Children and Families does oversee the health of illegal aliens caught at the border and brought to detention centers.
Speaking to NBC News last year, a spokesman for the HHS said those who pass through their program are provided missing childhood vaccinations.
Even doctors are worried about Obamacare. Here’s the advice from one top expert, on “Surviving the Medical Meltdown.”
“When children come into the Department of Health and Human Services program, they are given a well-child exam and given all needed childhood vaccinations to protect against communicable diseases,” said the spokesman.
Unaccounted for, however, are illegals who are not caught, do not enter detention centers or who are released by border agents within 72 hours of their capture.
Thirteen-year Border Patrol veteran Chris Cabrera is vice president of the Local 3307 chapter of the National Border Patrol Council, the exclusive representative of approximately 17,000 agents and support personnel assigned to the U.S. Border Patrol.
He recently said in a radio interview the Border Patrol is being overwhelmed by illegals, with many slipping through the cracks possibly carrying disease.
“It’s not always the ideal medical care,” Cabrera confessed, “and a lot of it is slipping through the cracks. I read now one of the publications this morning that [reported] they had a bunch of people go in there in at a detention facility [that] had to be shut down due to chicken pox.
“It’s kind of alarming, seeing as we toured that facility less than a month ago and they assured us that they had everything in order, that something like this wouldn’t happen. And sure enough, it fell through the cracks.”
“We’re not set up for this, and we’re inviting more problems,” he said.
Asked specifically whether he was referring to diseases slipping through the cracks, Cabrera said, “Medical problems, gang members that we’re releasing; they’re going to these cities, they’re not staying down here.
“So these problems are going to be coming to your town,” he said.
California: Ground zero for measles
From Jan. 1 to Feb. 6, 2015, 121 people from 17 states are reported to have had measles.
The CDC’s website stated, “Most of these cases are part of a large, ongoing multi-state outbreak linked to an amusement park in California.”
Anne Schuchat, director of the CDC’s National Center for Immunization and Respiratory Diseases, explained the “genotype of the virus that’s associated with the Disneyland outbreak is causing outbreaks in 14 different countries around the world.”
She fingered Indonesia, India and Dubai as possible sources under investigation but made clear her agency is still unsure of the exact origins of the outbreak.
“We assume that someone got infected overseas, visited the parks and spread the disease to others,” she said.
While medical literature backs up the argument that Latin America is currently safely immunized against measles, a WND review of the history of outbreaks in the U.S. since the 1980s shows two major themes: Almost all of the outbreaks came from overseas, and California saw some of the largest concentrations of the disease.
Since the current outbreak began in December, more than 100 people have been reported infected with the measles in California, data from California’s Department of Public Health shows. Such a concentration is unsurprising since the outbreak this year was said to have originated in the state.
A CDC graph of measles outbreaks since 2001 shows an alarming spike since 2014, when the U.S. experienced a record number of 644 cases from 27 states, with another major concentration in California.
From Jan. 1-April 18, 2014, the California Department of Public Health reportedly received 58 confirmed measles cases, the largest number the state has seen since 1995. The nationwide outbreak during that period was 129 reported cases.
Morbidity and Mortality Weekly reported that in the vast majority of all 58 cases in 2005, 54 were classified as “importation-associated,” including “13 importations, 13 cases epidemiologically linked to importations, 18 with virologic evidence suggesting recent importation and 10 linked to cases with virologic evidence of recent importation.”
The year 2011 saw another measles outbreak concentrated in California. On Aug. 26, 2011, the Los Angeles County Department of Public Health investigated a suspected measles outbreak originating in a refugee from Burma who had arrived on a flight bound for the city.
In May, 2011, Dr. Gilberto Chavez, deputy director of the Center for Infectious Diseases at the California Department of Public Health, announced, “California, like the rest of the nation and, indeed, the world, is experiencing an increase in measles cases that is entirely preventable with immunization.”
Morbidity and Mortality Weekly Report documented in 2008 that of the 64 measles cases between January and April of that year, “54 were associated with importation of measles from other countries into the United States.” That year saw another major confrontation in California, including one outbreak attributed to an unvaccinated boy from San Diego.
Outbreaks in 2006 were associated with a measles case in a Missouri resident who had recently traveled to China and a California woman returning from a trip.
In 2005, there were 66 confirmed cases of measles, with 34 of them said to have originated with a single outbreak in Indiana from an infected traveler returning to the U.S. An outbreak one year before was said to have originated with a University of California-Santa Cruz student who met a newly adopted toddler from China.
In 2005, three states accounted for 49 percent of cases: Washington, California and New York.
Data shows that during 2001-2003, a full 6 percent of the 216 reported measles cases were imported, and 120 were indigenous.
In 2000, Japan, Korea and Ethiopia amounted for the largest numbers of imported cases, with New York, California, Hawaii and Vermont the states with the most outbreaks.
Enterovirus
While Latin America has implemented a successful measles immunization program, the region is home to numerous epidemics currently sweeping America, including enterovirus, which has been responsible for at least 14 deaths since last year.
There has been speculation the polio-like enterovirus, which mostly targets children, could have been carried into the U.S. by illegal-alien minors from Central America.
The World Health Organization last September issued a global alert for the enterovirus 68, or EV-D68, in the U.S.
A global WHO alert for the virus is exceptionally rare and is the first of its kind associated with an outbreak in the U.S.
The last global alert for enterovirus was issued in 2008 in China. The only other enterovirus alert came 10 years earlier, in 1998, again in China.
As with measles, the enterovirus outbreak has taken on a political tone, with some suggesting the virus may have been carried to the U.S. by illegal aliens, especially the so-called unaccompanied alien children, or UACs, who have been streaming across the southern border.
Most UACs originate in Central American countries, some of which have seen recent spates of EV-68 virus outbreaks.
A study published Oct. 11, 2013, in Virology Journal collected nasopharyngeal swabs from eight Latin American countries from 3,375 subjects aged 25 years or younger who presented with influenza-like illness.
The study found human enteroviruses were identified in a staggering 3 percent of all subjects.
Former CBS News correspondent Sharyl Attkisson, writing at her personal website, surmised “the origin could be entirely unrelated,” but because the “CDC hasn’t suggested reasons for the current uptick or its origin,” some are questioning “whether the disease is being spread by the presence of tens of thousands of illegal immigrant children from Central America admitted to the U.S. in the past year.”
Talk-show host Michael Savage said the EV-D68 could have been brought to the U.S. by illegal aliens.
Savage, who earned a doctorate in epidemiology at the University of California at Berkeley, declared on his show last November: “For 20 years, I’ve been trying to warn America about the unscreened immigrants being brought in. Now, of course, it’s coming home to roost and the American people are being lied to by the Centers for Disease Transmission. They used to be the CDC; they’re now the CDT.”
The progressive activist organization Media Matters for America has weighed in on matter.
In a blog posting titled “Conservatives Falsely Blame Undocumented Children For Deadly Enterovirus,” Media Matters cites a statement it obtained from CDC spokeswoman Jeanette St. Pierre saying: “Currently, there is no evidence from testing at CDC that EV-D68 infections in the U.S. are a result of unaccompanied minors moving into the country.”
Illegals brought aggressive mosquito?
Did illegal aliens from Central America bring with them an aggressive mosquito discovered in recent months in California that is a known transmitter of debilitating and possibly deadly viruses?
Both the mosquito itself and many of the viruses that can be transmitted by the insect are endemic to Central America and have been found in Mexico.
The yellow fever mosquitoes were found Oct. 7 and 8 in the Los Angeles counties of Commerce and Pico Rivera. The next month, the same mosquito was found in San Francisco.
The mosquito, also known by its scientific name, Aedes aegypti, is an insect capable of spreading dengue fever, chikungunya, yellow fever viruses and other diseases.
Susanne Kluh, director of scientific-technical services for the Greater Los Angeles County Vector Control District, told the Times that while the “debilitating viruses, so far, aren’t locally transmitted in L.A. County, the mosquitoes that can transmit them are now here.”
“Infected travelers can bring these viruses to Los Angeles County,” Kluh warned.
The Times reported that determining how the Aedes species were introduced to California has been difficult. Officials, the paper said, blame imported tires and plants, but it also can travel via planes, ships and other vehicles.
Like scores of other establishment media outlets covering the story, the L.A. Times failed to note the yellow fever mosquitoes, which are thought to have originated in Africa, are now present in tropical areas such as Central and South America and the northeast coast of Mexico.
The insects’ presence in Latin America means the mosquitoes or their eggs could just as easily have been transported into the U.S. in baggage, clothing, food, or liquids carried by illegal aliens crossing the border.
The female mosquitoes can lay up to 300 eggs at a time, with the future progeny usually deposited in clusters. Eggs are usually laid on the surface of stagnant water and can hatch in as little as an inch of standing water.
Further, many of the viruses that can be transmitted by the mosquito, such as chikungunya, which brings paralyzing joint pain, and yellow fever have been ravaging not only Africa but also Latin America and Central America.
The World Health Organization’s global alert on yellow fever, for example, documents the disease is “endemic in 10 South and Central American countries and in several Caribbean islands.”
“The disease was originally imported into the Americas from Africa, but became widely established there,” the alert adds.