CDC Agrees to Florida Ebola Preparedness Requests — To little to late? Déjà vu Pandemic?
The first line of defense against the spread of infectious diseases like Ebola is sealing the U.S. borders. The second line of defense, once the border is breached by omission or commission, is Florida’s hospitals. We can learn important lessons from another recent and ongoing pandemic – HIV/AIDS. HIV/AIDS and Ebola are pandemics. Both are transmitted by physical contact. Both kill horribly. Both could have been stopped from reaching our shores. Neither was.
Are we making the same mistakes twice? Is this a case of “Déjà vu Pandemic?”
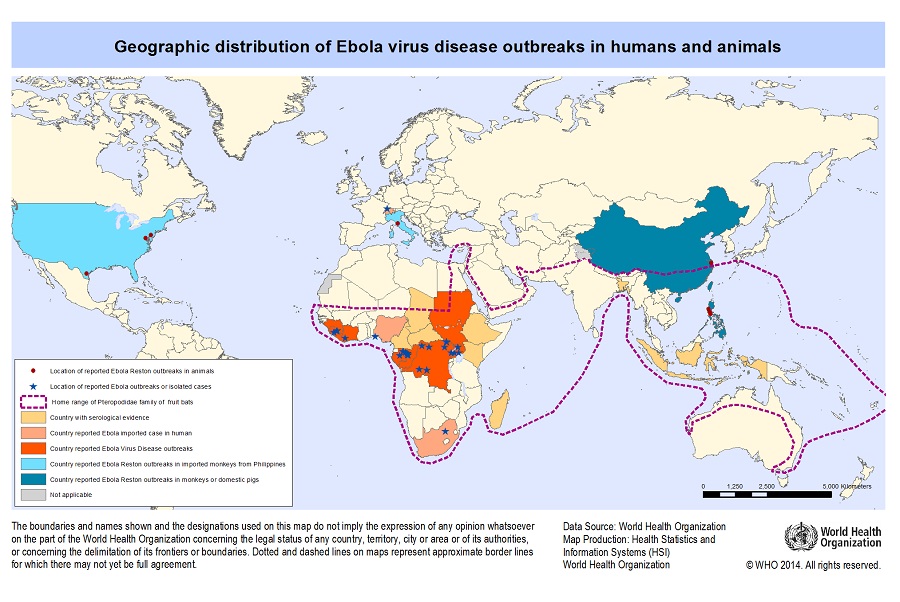
A new study of the spread of the HIV/AIDS virus shows that the disease’s origin was in the small town of Kinshasa, Congo. National Geographic’s Brandon Keim reports, “As the Ebola epidemic spreads, new information has emerged on the origins of a far more deadly killer. A new family history of the HIV virus that causes AIDS, reported Thursday [October 2, 2014], is troubling but instructive: Modernization in mid-20th-century Africa, especially in the city Kinshasa, played a profound role in shaping that global epidemic.”
How did the HIV/AIDS virus initially spread in Africa? Via their rail system, eventually reaching the shores of the U.S by boat and by plane.
While public support for a travel ban on countries with the Ebola virus grows, President Obama refuses to implement any such travel ban. On October 16, 2014 The Daily Signal’s Rob Bluey reported that U.S. Embassies in Ebola-stricken countries are still processing visas for non-U.S. citizens.
Accuracy in Media’s Cliff Kincaid in his column “Seeing Ebola Through Obama’s Eyes” writes:
The nephew of the black African who brought Ebola to the United States doesn’t blame his uncle. He blames us. He writes in The Dallas Morning News that his uncle did everything right in Liberia, but still got Ebola, and wasn’t treated correctly in the U.S. The claim is that he had a right to be on U.S. soil and that it’s our fault he’s dead.
I suspect this is how President Barack Obama views Ebola. How else do you explain his opposition to a common-sense ban on travel to the U.S. by people from Ebola-infected countries?
Tragically, Obama’s alternative is for the U.S. to become infected. Then, he must figure, there will be more pressure to find a “cure,” or at least a vaccine. But who knows how many will die in the process? It could be hundreds, or thousands, or more.
Florida Governor Scott announced that the CDC has agreed to two of the state’s requests for enhancing Florida’s Ebola preparedness efforts, including holding a conference call with healthcare workers on best practices and federal approval of the state’s repurpose of more than $7 million in federal grant funding. The CDC, has still not provided the additional 27 testing kits, or contacted the passengers that flew on the Frontier flight from Dallas to Ft. Lauderdale.
Governor Scott said:
“We want to thank the CDC for agreeing to hold a conference call with Florida hospitals on Monday, October 20th at 3:30 p.m. Our healthcare workers need to hear directly from the CDC on what happened in Dallas that allowed Ebola to be transmitted to two nurses, and what can be done to protect our healthcare professionals in Florida who are on the front lines. Florida hospitals also have questions of their own and the CDC must provide guidance.
“We appreciate the CDC’s preliminary approval to move forward with redirecting more than $7 million in federal grant funds to purchase the necessary equipment and supplies to protect healthcare workers who may come into contact with Ebola. The CDC indicated that we will receive formal approval next week, but based on this preliminary approval, we have already begun using these funds to enhance our Ebola preparedness efforts.
“While this is great progress, we’re waiting on the CDC to provide additional testing kits. With a population of more than 19 million people, tens of millions of tourists, and numerous ports and international airports, we must ensure Florida can rapidly test any future patients who have the potential for Ebola.
“The CDC still needs to identify, notify, and monitor all of the passengers that flew from Dallas to Ft. Lauderdale after nurse Amber Joy Vinson flew on the same plane. We know she had a low grade-fever when she traveled to Dallas, and the plane then came to Florida. While this risk is low, there have been reports she was potentially symptomatic, and the CDC should take any potential threat seriously – no matter how small. We’re continuing to hope for the best, while preparing for the worst and we expect the CDC to do everything possible to ensure our communities are kept safe.”
The CDC has agreed to hold a conference call with Florida hospitals on Monday, October 20th at 3:30 p.m. This call will cover critical areas of preparedness and training for our Florida hospitals. Officials with the CDC’s state and local readiness section will be hosting the call with Florida’s hospital executives. The call will provide guidance for proper use of Personal Protective Equipment (PPE), safe handling of medical waste and effective clinical strategies within the hospital setting.








 Yulia Latynina
Yulia Latynina